what are the issues related to concepts, models and theories of advanced practice nursing?
Chapter two
Conceptualizations of Advanced Do Nursing
Why are conceptualizations of advanced do nursing of import for students and practicing advanced practice nurses (APNs) to understand? The content may seem dry to students, who are otherwise excited about learning new ways of caring for individuals, through their APN teaching. Concepts, models, and theories seem remote from the existent work of eliciting histories, performing physicals, planning handling, evaluating outcomes, and otherwise helping patients and families improve their health, cope with illnesses, and die with dignity. Whether one does so consciously, all these advanced do activities are guided by some model or framework. Novices may rely more frequently on rules and guidelines to accomplish their piece of work. Skilful APNs may not consult rules and guidelines for common problems, simply tin improvise new ways of thinking (models) when faced with novel situations. Regardless of years of experience, APNs rely on common processes and linguistic communication in their communications with colleagues near patient care and recognize when they must explain a clinical situation to someone unfamiliar with the patient. Similarly, information technology is important for the nursing profession and for private APNs to understand the linguistic communication of advanced do nursing to communicate with each other, clients, and stakeholders. Currently, converging forces in the United States are moving rapidly, requiring the profession to advance a mutual understanding of advanced practise nursing, which is likely to inform hereafter conceptualizations of advanced practice nursing.
The development of a mutual language and conceptual framework for communication and for guiding and evaluating do, education, policy, inquiry, and theory is primal to sound progress in any practice discipline. Given the evolving changes in the U.South. health intendance system, such a foundation is especially crucial at this stage in the development of advanced practice nursing. Since the concluding edition, a professional person consensus on advanced practise nursing regulation has been reached in the United States—the Consensus Model for APRN Regulation (2008) and is existence implemented. In improver, the Plant of Medicine [IOM] (2011) has chosen for integrating advanced practice nursing more completely into the U.South. health care delivery system. Other forces driving a common understanding of advanced practice nursing are the expansion of programs offering the Doctorate of Nursing Do (DNP), the Patient Protection and Affordable Care Act (PPACA, 2010), accountable care organizations, and the promulgation of interprofessional competencies (Canadian Interprofessional Health Collaborative [CIHC], 2010; Health Professions Networks, Nursing and Midwifery, & Human Resource for Health, 2010; Interprofessional Education Collaborative [IPEC] Proficient Panel, 2011) and pedagogy (see Capacity 12 and 22). Agreement what advanced do nursing is, what APNs practice, similarities and differences among APNs, and how APNs contribute to affordable, attainable, and effective intendance is central to the redesign of U.S. health care. Information technology is important for readers to sympathise that because of the dynamic and evolving nature of health care reform and nursing organizations' activities in this arena, nationally and globally, the content in this affiliate is irresolute chop-chop. Readers are encouraged to consult the websites cited in this affiliate for up to date data.
Internationally, there have been efforts to clarify, establish, and/or regulate avant-garde practise roles inside the nursing profession in other countries (eastward.g., Canadian Nurses Association [CNA] 2007, 2008, 2009a, b; International Quango of Nurses [ICN] (2009). In countries in which APN roles be, in addition to studies of the distinctions amid roles (Gardner, Chang, & Duffield, 2007; Gardner, Gardner, Middleton, et al., 2010), efforts are underway to establish educational programs (Wong, Peng, Kan, et al., 2009) or develop frameworks that clarify education, scope of do, registration and licensing, and/or credentialing that are land-specific (e.k., Fagerström, 2009). Statements by national organizations such every bit the CNA and ICN and manufactures on conceptualizations of advanced practice nursing proposed by authors from other countries (e.one thousand., Brawl & Cox, 2004; CNA, 2007, 2008, 2009a, b; DiCenso, Martin-Misener, Bryant-Lukosius, et al., 2010; Gardner, Chang, & Duffield, 2007; Gardner et al., 2010; Mantzoukas & Watkinson, 2007; McMurray, 2011; Pringle, 2010) take been reviewed. Although contextual factors may differ from those in the U.s.a., at that place are global opportunities for clarifying and advancing avant-garde do nursing and these should be specific to a land's culture, health system, professional standards, and regulatory requirements. Content from manufactures about advanced practice in other countries is used to present models or illuminate certain conceptual issues; they as well inform the give-and-take of recommendations and futurity directions. For a more than complete give-and-take of global perspectives on advanced do nursing, meet Chapter six.
In reviewing the literature for this edition, searches were conducted using the terms advanced practice nursing, model, or theory, and the four APN roles. In improver, a search was done of the authors of models cited in the prior edition. Few new curricular models were identified (Fagerström, 2009; Perraud, Delaney, Carlson-Sabelli, et al., 2006; Wong et al., 2009), merely several types of articles related to model development, model testing, and models used in advanced practise nursing were identified. These models may be characterized as follows:
• Curriculum models (e.g., Fagerström, 2009; Perraud et al., 2006; Wong et al., 2009)
• Administrative or organizational models (e.chiliad., Ackerman, Mick, & Witzel, 2010; Scarpa & Connelly, 2011; Skalla & Caron, 2008)
• Models that differentiate among avant-garde practice roles (e.one thousand., Gardner, Chang, & Duffield, 2007)
• Models of the nature of advanced practice nursing (e.one thousand., Brawl & Cox, 2003; Brown, 1998; Hamric, 1996, 2009, and see Chapter three; Mantzoukas & Watkinson, 2007; Styles & Lewis, 2000)
• Models that differentiate between bones and advanced practice nursing (due east.k., Calkin, 1984; Oberle & Allen, 2001)
• Models of role evolution of APNs (see Chapter four)
• Models of APN regulation and credentialing (e.1000., the APRN [Advanced Exercise Registered Nurse] Consensus Model, 2008; CNA, 2007, 2008, 2009a, b; Stanley, Werner, & Apple, 2009; Styles, 1998);
• Models of interdisciplinary practice (Dunphy & Winland-Chocolate-brown, 1998; Dunphy, Winland-Dark-brown, Porter, Thomas, & Gallagher, 2011);
• Models that APNs would discover useful include the following:
 Awarding or testing of grand and center-range theories to APN exercise (east.g., Musker, 2011; Newcomb, 2010);
Awarding or testing of grand and center-range theories to APN exercise (east.g., Musker, 2011; Newcomb, 2010);
 Models of role implementation (Brawl & Cox, 2004; Bryant-Lukosius, DiCenso, Browne, & Pinelli, 2004) and APN intendance delivery (Mahler, 2010; McAiney, Haughton, Jennings, et al., 2008; Dunphy & Winland-Brown, 1998; Dunphy, Winland-Brown, Porter, Thomas, & Gallagher, 2011; Curley, 1998; American Clan of Critical Care Nurses, 2012)
Models of role implementation (Brawl & Cox, 2004; Bryant-Lukosius, DiCenso, Browne, & Pinelli, 2004) and APN intendance delivery (Mahler, 2010; McAiney, Haughton, Jennings, et al., 2008; Dunphy & Winland-Brown, 1998; Dunphy, Winland-Brown, Porter, Thomas, & Gallagher, 2011; Curley, 1998; American Clan of Critical Care Nurses, 2012)
• Models to evaluate outcomes of advanced nursing practice (run into Chapters 23 and 24).
In addition, professional organizations with interests in licensing, accreditation, certification, and educational (LACE) issues regarding APNs tin be viewed as operating from some conceptualization of advanced practice nursing, whether implicit or explicit. In this affiliate, the post-obit types of models will exist discussed: those promulgated past APN stakeholder organizations, models that describe the nature of advanced do and/or differentiate between avant-garde and basic exercise, and selected models that APNs may find useful in practice.
In previous editions, problems associated with lack of a unified definition of advanced practice and imperatives for undertaking this important work were identified. When practicable, consensus on advanced do nursing models should be beneficial for patients, club, and the profession. Although the APRN Consensus Model (2008) has brought needed conceptual clarity to regulation of avant-garde exercise nursing in the United States, there is still piece of work to be done with regard to other aspects of conceptualizing avant-garde practice nursing, such as APN competencies, differentiating basic and advanced nursing practice, and differentiating the avant-garde practice of nursing from the practices of other disciplines. This work has become more urgent given the impacts of other U.S. initiatives that are unfolding. I have reviewed published documents from national professional organizations and the literature and focused selectively on models of APN exercise. This review is not exhaustive. For example, in limiting the scope of this chapter, statements on advanced practice nursing by specialty organizations have not been examined. Thus, the purposes of this chapter are as follows:
Readers are invited to debate and enlarge on the models, issues, and thinking put frontwards in this chapter.
Nature, Purposes, and Components of Conceptual Models
A conceptual model is 1 part of the structure, or holarchy, of nursing knowledge. This construction consists of metaparadigms (most abstract), philosophies, conceptual models, theories, and empirical indicators (most concrete; Fawcett, 2005). Traditionally, key concepts in the metaparadigm of nursing, which nursing theories are expected to accost in their conceptual underpinnings, are humans, the surround, health, and nursing (Fawcett, 2005). Although some theorists have proposed boosted or expanded concepts, Fawcett's ideas inform this discussion. At this stage of the evolution, conceptual models of avant-garde practice nursing remain an appropriate focus.
A number of answers to these questions are in the nursing literature. Fawcett (2005) has identified a conceptual model as "a gear up of relatively abstract and general concepts that address the phenomena of central interest to a discipline, the propositions that broadly describe these concepts, and the propositions that state relatively abstract and general relations between 2 or more than of the concepts" (p. 16).
Fawcett (2005) also noted that a conceptual model is "a distinctive frame of reference…that tells [adherents] how to detect and interpret the phenomenon of interest to the discipline" and "provide alternative ways to view the subject affair of the bailiwick; there is no 'best' way." Although there is no best way to view a phenomenon, evolving a more than uniform and explicit conceptual model of advanced do nursing is likely to benefit patients, nurses, and other stakeholders (IOM, 2011) and have applied benefits. It tin facilitate communication, reduce conflict, ensure consistency of advanced exercise nursing, when relevant and appropriate, across APN roles, and offering a "systematic approach to nursing research, educational activity, assistants, and practice" (Fawcett, 2005). Thus, conceptual models serve many purposes.
Models may assist APNs articulate professional role identity and function, serving as a framework for organizing beliefs and cognition about their professional roles and competencies, providing a basis for farther development of knowledge. In clinical do, APNs use conceptual models in the delivery of their holistic, comprehensive, and collaborative care (eastward.g., Carron & Cumbie, 2011; Dunphy & Winland-Brown, 1998; Dunphy et al., 2011; Musker, 2011). Models may also be used to differentiate amid levels of nursing practice—for case, between staff nursing and advanced practice nursing (Calkin, 1984; ANA, 2010b). In research and other scholarly activities, investigators apply conceptual models to guide research and theory evolution. An investigator could decide to focus on the written report of one concept or examine relationships among select concepts to elucidate testable theories. For example, research by Fenton (1985) and Brykczynski (1989) has elucidated new domains of exercise for clinical nurse specialists (CNSs) and nurse practitioners (NPs), respectively. In educational activity, kinesthesia use conceptual models to programme curricula, identify important concepts and the relationships among them, and brand choices about grade content and clinical experiences for preparing APNs (Perraud et al. 2006; Wong et al., 2009).
Fawcett and colleagues (Fawcett, Newman, & McAllister, 2004; Fawcett & Graham, 2005) have raised additional conceptual questions about advanced practice:
Because direct clinical practice is viewed every bit the fundamental APN competency, 1 could also ask: "What does the term clinical mean? Does it refer simply to hospitals or clinics?" These questions are becoming more important given the APRN Consensus Model and given the role that APNs are expected to play across the continua of health intendance equally a result of the PPACA and its reforms. From a regulatory standpoint, the emphasis on a specific population every bit a focus of practice will lead, when appropriate, to reconceptualizing curricula to ensure that graduates are prepared to succeed in new or revised certification examinations. Hamric (see Chapter 3) has noted that some APN competencies are likely to be performed past nurses in other roles only suggests that the expression of these competencies by APNs is different. For example, all nurses collaborate but a unique aspect of APN practice is that APNs are authorized to initiate referrals and prescribe treatments that are implemented by others (e.m., physical therapy). Innovations and reforms arising from the PPACA volition ensure that APNs are explicitly engaged in the delivery of intendance across care settings, including in nursing clinics and palliative care settings, and as full participants in interprofessional teams. Changes in regulations and in the delivery of health care must and should lead to new or revised conceptualizations of avant-garde practice nursing, such as defining theoretical and evidence-based differences between APN care and the intendance offered by other providers and clinical staff, the role of APNs in interprofessional teams, and specialization and subspecialization in advanced do nursing. This piece of work will enable nursing leaders and health policy makers to design a health care system that delivers high-quality intendance at reasonable toll based on disciplinary and interdisciplinary competencies, outcomes, effectiveness, efficacy, and costs. Indeed, this textbook reflects a consistent attempt to evaluate and revise the authors' conceptualizations of advanced practice nursing based on current contextual factors. The conceptualization advanced in this text has been remarkably stable since it was beginning proposed in 1996 and has required small modifications as APN roles and health intendance have evolved.
In addition to a pragmatic reevaluation of advanced exercise nursing concepts based on the evolution of APN regulation and health care reform, writers in the United States and away are raising important theoretical questions well-nigh conceptualizations of advanced practice, including the post-obit: the epistemologic, philosophical, and ontologic underpinnings of advanced practice (Arslanian-Engoren, Hicks, Whall, & Algase, 2005); the nature of advanced practice noesis, discerning the differences betwixt and among the notions of specialty, avant-garde practice, and advancing practice (Allan, 2011; Christensen, 2009, 2011; Macdonald, Herbert, & Thibeault, 2006; Thoun, 2011); and the extent to which APNs are prepared to study and apply nursing theories in their practices (Algase, 2010; Arslanian-Engoren, Hicks et al., 2005; Karnick, 2011).
In summary, questions arising from a irresolute health policy landscape and from theorizing about avant-garde exercise nursing point to the need for well idea-out, robust conceptual models to help individuals answer of import questions about the phenomenon—in this instance, avant-garde do nursing. The need for clarity almost advanced practice nursing, what information technology is and is not, is condign more important, not but for patients and those in the nursing profession only for evolving initiatives such as interprofessional education (CIHC, 2010; Health Professions Networks, 2010; IPEC Expert Panel, 2011), practice (American Association of Nurse Anesthetists, 2012), and creation of accountable care organizations, efforts to build teams and systems in which constructive advice, collaboration, and coordination lead to quality intendance and improved patient, institutional, and fiscal outcomes.
Conceptualizations of Advanced Practice Nursing: Problems and Imperatives
Despite the usefulness and benefits of conceptual models, some difficulties are apparent in the literature when the clinical and professional issues inherent to advanced practice nursing are examined. Although there is increasing conceptual clarity about avant-garde practise nursing, five issues of conceptual defoliation or dubiety in the development of advanced practice nursing can yet exist identified.
Despite improvements in the area of regulation, the first issue remains the absence of well-defined and consistently applied terms of reference. A core stable vocabulary, a lingua franca, is needed for definition and model building. The lack of a consistent stable vocabulary can be seen in the literature. Shuler and Davis (1993a) accept stated that "One of the greatest barriers to using nursing models in [nurse practitioner] practice relates to vocabulary and communication…." Despite progress, this challenge remains. For example, in the United States, advanced exercise nursing is the term that is used but the ICN and CNA utilize the term avant-garde nursing do. Furthermore, the role and functions of APNs could be better conceptualized. Although the apply of competency is becoming more common, concepts most APN work are variously termed roles, hallmarks, competencies, functions, activities, skills, and abilities. Few models of APN do address nursing's metaparadigm (person, wellness, environs, nursing) comprehensively. The problem in comparison, refining, or developing models is that terms are used with no universal pregnant or frame of reference; occasionally, no definition is offered at all, or terms are used inconsistently. This instability and inconsistency are axiomatic in many models cited in this affiliate. It is rightly anticipated that conceptual models of the field and its do change over time. However, the evolution of avant-garde exercise nursing and its comprehension by nurses, policymakers, and others volition be enhanced if scholars and practitioners in the field agree on the use and definition of fundamental terms of reference.
The second issue is that many attempts to articulate models of advanced practice nursing fail to consider extant literature that is directly relevant to such conceptualizing activities. In part, this may be a upshot of the lag between the conceptualizing try and its ultimate publication, the knowledge explosion, and the role of the Net and social media in the generation and dissemination of knowledge. For case, some recently published articles reviewed for this affiliate cited work from the 1980s and 1990s; revised publications of these before cited works, although apparently available, were non cited. This caution should be considered when proposing, evaluating, or refining advanced practice nursing models.
The 3rd issue is a lack of clarity regarding conceptualizations that differentiate between and amid levels of clinical practice:
Although many authors who write almost advanced practice nursing cite Benner's model of skilful practise (1984), they rarely signal that the model was derived from the study of nurses who were primarily experts by experience, not APNs. Certainly, Benner'south model is relevant to efforts to conceptualize advanced practise nursing, as demonstrated past Fenton'due south (1985) and Brykczynski's (1989) work. Given that clinical practice is why the profession of nursing exists and is central to advanced practise nursing, models that assistance the profession differentiate levels of practice are needed.
The fourth issue is the need to analyze the differences between advanced practice nursing and medicine (meet Chapter 3). Graduate APN students struggle with this issue as part of role evolution (see Affiliate iv). This lack of conceptual clarity is apparent in advertisements that invite NPs or physician assistants to apply for the same job. As noted in Capacity 21 and 22, organized medicine expends resource in trying to limit or ignominy avant-garde practice nursing, even as some physician leaders work on behalf of advocating for APNs. Hamric, in Chapter iii, asserts that advanced practise nursing is non the junior practice of medicine, an exclamation supported by the seven competencies of advanced do nursing (Chapters 7 through 13). Fawcett, a well-respected nursing leader, has asked, "What does information technology mean to blend nursing and medicine?" (Fawcett et al., 2004; Fawcett & Graham, 2005). Finally, little is understood near the impact of APN-doctor collaboration on do or about strategies for matching the level of knowledge and skill to the needs of patient populations (Brooten & Youngblut, 2006; Calkin, 1984).
The fifth issue is interprofessional instruction and practice, a concept that is cardinal to accountable, collaborative, coordinated, and high-quality care. The development of interprofessional competencies for health professionals (CIHC, 2010; Health Professions Networks, 2010; IPEC Expert Panel, 2011) suggests that the more of import questions now are not virtually "blending" APN and doc practice, but questions such as "How practice nosotros ensure that despite differing disciplinary backgrounds, patients, colleagues, and other observers recognize the behavioral expressions of interprofessional competencies?" Also, how do we undertake the conceptual, curricular, credentialing, and other work that will exist needed to make interprofessional practice and constructive teamwork the gold standard of quality care? The existence of interprofessional competencies and emergence of promising conceptualizations of interprofessional work. (e.g., Barr, Freeth, Hammick, et al., 2005; Reeves, Goldman, Gilbert, et al., 2011) are critical contextual factors for elucidating and advancing conceptualizations of advanced practise nursing. See Chapter 12.
Among many imperatives for reaching a conceptual consensus on advanced exercise nursing, about of import are the interrelated areas of policymaking, licensing and credentialing, and practice, including competencies. In the policymaking arena, for instance, not all APNs are eligible to be reimbursed by insurers, and even those activities that are reimbursable are oftentimes billed incident to a physician's care, rendering the work of APNs invisible. The APRN Consensus Model (2008), the PPACA, and the IOM's call for changes to enable APNs to work inside their full scope of practice (IOM, 2011). will arrive easier for U.Southward. policymakers to recommend and adopt changes to policies and regulations that now constrain APN practice, somewhen making the contributions of APNs to quality intendance visible and reimbursable. Agreement on vocabulary and concepts such as competencies that are common to all APN roles will maximize the ability of APNs to work within their full scope of practice.
Although some progress has been made, at that place are compelling reasons for standing dialogue and activity aimed at clarifying avant-garde exercise nursing and the concepts and models that assist stakeholders understand the nature of APN work and their contributions. Reaching consensus on concepts and vocabulary will serve theoretical, applied, and policymaking purposes. As the work of wellness care reform and implementing interprofessional competencies, educational activity, and practice moves frontward, there will be opportunities for the profession to conceptualize advanced do nursing more than clearly. Description and consensus on conceptualization of the nature of advanced exercise nursing will lead to the following outcomes:
Conceptualizations of Avant-garde Practice Nursing Roles: Organizational Perspectives
Practise with individual clients or patients is the central work of the field; it is the reason for which nursing was created. The following questions are the kinds of questions a conceptual model of advanced practice nursing should reply:
Some conceptual models reviewed in this chapter are more narrowly focused than others. Some advanced practice models are more than homogeneous and some are mixed with respect to the phenomenon studied. Some could be seen every bit micromodels in terms of the unit of measurement of analysis and others could exist seen every bit metamodels, incorporating a number of conceptual frameworks. Some models explain systems; others explicate relationships between and among systems. All these foci are important, depending on the purposes to be served. However, in the development of conceptual models, the phenomenon to exist modeled must be carefully divers. For example, is the model intended to embrace the entire field of avant-garde do nursing, or is it confined to distinctive concepts such equally collaborative practice between physicians and APNs? Is advanced nursing practise different from advanced practice nursing? If a phenomenon and its related concepts are not conspicuously defined, the model could exist and so inconsistent as to be confusing or so comprehensive that its impact volition be diluted.
In addition to describing concepts and how they are related, assumptions about the philosophy, values, and practices of the profession should exist reflected in conceptual models. The nowadays give-and-take of conceptualizations of advanced practice nursing is guided past 3 assumptions:
In the next department, the implicit and explicit conceptualizations of avant-garde do nursing promulgated by professional organizations concerned with defining APN practice and with clarifying particular APN roles are discussed. Organizations such as the Oncology Nursing Club and the American Clan of Critical-Care Nurses [AACN]) accept addressed advanced practice nursing in their specialties. Although specialty models and standards are important to students and APNs, they are non addressed in this chapter. Every bit students and readers consider their own APN practices, they may want to review the history of avant-garde do nursing (see Chapter 1) and evolving advanced practice nursing roles (see Chapter 5) to inform their efforts to conceptualize their own practices.
Although not all the documents described in this section are conceptual models, many imply, describe, or reference a conceptual framework. The APRN Consensus Model (2008) represents a major stride forrad in promulgating a uniform definition of advanced practise nursing, for the purposes of regulation, in the Usa. This achievement is informing efforts past other organizations; even so, some issues with the absence of a cadre vocabulary noted earlier are credible as ane reads the unlike approaches taken by other professional organizations; therefore, comparisons are difficult to make because terms of reference and their meanings vary. To help the reader appreciate the challenge of developing a common language to narrate advanced practice nursing, lexicon definitions of terms used in conceptualizations of advanced practice nursing are establish in Box ii-1. In spite of differences in terminology, the efforts of the profession to deal with a definition of advanced practise nursing are evident in the documents reviewed hither. Reflection on and give-and-take of the various terms used, and contend about interpreting terms such as roles, domains, and competencies, may contribute to the clarification of conceptual models and the emergence of a common language. The descriptions of each model in the following sections are necessarily express. The reader is encouraged to refer to the original documents and organizations' websites to understand advanced practice nursing as described past organizations and individual authors more fully. Website addresses for national APN organizations are found in Chapter 21. The APRN Consensus Model, the upshot of collaboration of many organizations, is described first, considering it will proceed to guide and influence conceptualizations of avant-garde practise, at least with regard to regulation and credentialing, for the most future.
Box ii-i
Definition of Terms
Competent Having requisite or acceptable ability or qualities; legally qualified or adequate; having the capacity to function or develop in a detail fashion (sufficient)
Competence, competency The quality or state of being competent; the knowledge that enables a person to speak and understand a language
Component A constituent part; ingredient
Domain A sphere of knowledge, influence, or activity
Role A socially expected behavior pattern usually determined by an individual'southward status in a item society
Hallmark Distinguishing characteristic, trait, or feature
Sphere An area or range over or within which someone or something acts, exists, or has influence or significance
Scope Infinite or opportunity for unhampered motility, activity, or thought; extent of treatment, activity, or influence
Standard Something established by authority, custom, or full general consent as a model or example; something set upwardly and established by an potency as a rule for the measure of quantity, weight, extent, value, or quality
Adapted from Mish, F.C. (Ed.). (2001). Merriam-Webster'southward collegiate lexicon. (10th ed.). Springfield, MA: Merriam-Webster International; and American Association of Colleges of Nursing (AACN). (2006). The essentials of doctoral teaching for advanced nursing practice (www.aacn.nche.edu/publications/position/DNPEssentials.pdf).
Consensus Model for Advanced Practise Registered Nurse Regulation
In 2004, an APN Consensus Conference was convened, based on a request from the American Association of Colleges of Nursing (AACN) and the National System of Nurse Practitioner Faculties (NONPF) to the Brotherhood for APRN Credentialing. The purpose was to develop a procedure for achieving consensus regarding the credentialing of APNs (APRN Consensus Model, 2008; Stanley, Werner, & Apple tree 2009) and the development of a regulatory model for advanced practice nursing. Independently, the APRN Advisory Committee for the National Council of State Boards of Nursing (NCSBN) was charged by the NCSBN board of directors with a similar task of creating a future model for APRN regulation and, in 2006, disseminated a draft of the APRN Vision Newspaper (NCSBN, 2006), a document that generated debate and controversy. Within a yr, these groups came together to form the APRN Articulation Dialogue Group, with representation from numerous stakeholder groups, including AACN, NCSBN, and organizations representing APNs. The outcome was the APRN Consensus Model (2008).
The APRN Regulatory Model includes important definitions, the roles and titles to be used, and population foci. Furthermore, it defines specialties and describes how to make room for the emergence of new APRN roles and population foci inside the regulatory framework. In addition, a timeline for adoption and strategies for implementation were proposed, and progress has been made in these areas (come across Chapter 21 for further information; only the model is discussed hither). Figure 2-one depicts the components of the APRN Consensus Model, the iv recognized APN roles and six population foci. The term advanced practice registered nurse (APRN) refers to all 4 APN roles. An APRN is defined as a nurse who meets the following criteria (APRN Consensus Model, 2008):
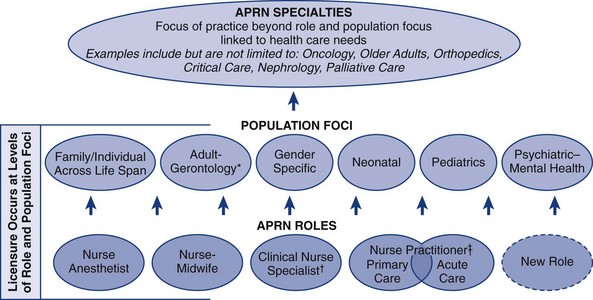
FIG 2-ane Consensus model for APRN regulation. This model was based on the work of the APRN Consensus Work Group and the NCSBN APRN Informational Committee. (From APRN Articulation Dialogue Group. [2008]. Consensus Model for APRN Regulation. [world wide web.aacn.nche.edu/pedagogy-resource/APRNReport.pdf]).*The population focus Adult-Gerontology encompasses the immature adult to the older adult, including the frail elderly. APRNs educated and certified in the Adult-Gerontology population are educated and certified across both areas of do and will be titled Adult-Gerontology CNP or CNS. In addition, all APRNs in any of the 4 roles providing care to the adult population (e.grand. Family or Gender Specific) must be prepared to come across the growing needs of the older adult population. Therefore the teaching program should include didactic and clinical education experiences necessary to prepare APRNs with these enhanced skills and knowledge.†The clinical nurse specialist (CNS) is educated and assessed through national certification processes across the continuum from wellness through acute intendance.‡The certified nurse practitioner (CNP) is prepared with the astute care CNP competencies and/or the primary intendance CNP competencies. At this point in time the acute intendance and master care CNP delineation applies simply to the Pediatrics and Adult-Gerontology CNP population foci. Scope of do of the principal care or acute care CNP is non setting-specific merely is based on patient care needs. Programs may ready individuals across both the primary care and acute care CNP roles. If programs fix graduates across both roles, the graduate must be prepared with the consensus-based competencies for both roles and must successfully obtain certification in both the acute and the primary care CNP roles.
The definition of the components of the APRN Consensus Model begins to address some of the questions nearly advanced practice posed earlier in this affiliate. An important understanding was that providing straight care to individuals is a defining feature of all APRN roles. This agreement affirms a position long held past editors of this text—that when at that place is no direct do component, one is not practicing equally an APN. It also has of import implications for LACE and for career development of APNs.
Graduate pedagogy for the four APRN roles was described in the consensus document. It must include completion of at to the lowest degree three separate, comprehensive graduate courses in advanced physiology and pathophysiology, wellness cess, and advanced pharmacology, consistent with requirements for the accreditation of APN instruction programs. In add-on, curricula must accost 3 other areas—the principles of decision making for the particular APN role, training in the core competencies identified for the role, and role preparation in one of the six population foci.
The Consensus Model asserts that licensure must be based on educational grooming for one of the four existing APN roles and a population focus; certification must be inside the aforementioned expanse of study; and that the four split processes of LACE are necessary for the adequate regulation of APRNs (APRN Consensus Model, 2008; come across Chapter 21). The half dozen population foci displayed in Effigy 2-1 include the individual and family across the life span, including developed, gerontologic, neonatal, pediatric, women's health/gender-specific, and psychiatric and mental health populations. Preparation in a specialty, such as oncology or disquisitional intendance, cannot be the basis for licensure. Specialization "indicates that an APRN has additional cognition and expertise in a more detached area of specialty practice. Competency in the specialty area could be acquired either by educational preparation or experience and assessed in a variety of ways through professional credentialing mechanisms (e.thou., portfolios, examinations)" (APRN Consensus Model, 2008, p. 12). This was a critical decision for the group to reach, given the numbers of specialties and APN specialty examinations in place when the certificate was prepared.
With this brief overview of the APRN Consensus Model, one can ask how this model has advanced the conceptualization of advanced practice nursing. Information technology is helpful for many reasons. First, for the U.s., information technology affirms that there are 4 APN roles. Second, it is advancing a uniform approach to LACE and advanced practice nursing that will have many applied and policymaking effects, including better alignment between and among APN curricula and certification examinations. Although non comprehensively described, it begins to accost the consequence of differentiating between RNs and APNs and will exist foundational to time to come efforts to differentiate amongst nursing roles. By addressing the issue of specialization, the model offers a reasoned arroyo for the following: (i) avoiding confusion that would arise from a proliferation of specialty certification examinations; (2) ensuring that considering of a limited and parsimonious focus (four roles and six populations), there volition be sufficient numbers of APNs for the relevant examinations to ensure psychometrically valid data on exam results; and (three) allowing for the development of new APN roles or foci to see society's needs.
What are the limits of this conceptualization of advanced practice nursing? Start, competencies that are common across APN roles are not addressed across defining an APRN and indicating that students must be prepared "with the core competencies for i of the four APRN roles across at least one of the six population foci" (APRN Consensus Model, 2008). However, every bit the Hamric Model suggests (see Chapter 3), there are core competencies that all APNs should possess. In addressing specialization, the model also leaves open up the upshot of the importance of educational preparation, in addition to experience, for advanced do in a specialty. Experience in an area is certainly a gene that leads to the emergence of new specialties, only volition experience lone be sufficient for the APN who specializes in oncology or critical care (or some other specialty) to achieve desired outcomes in timely and toll-effective ways? These are specialties in which the population's needs are many and circuitous and the scope of research noesis is similarly broad and deep. These are important conceptualization questions that are probably best addressed by the ANA and specialty professional nursing organizations, rather than by a group with a regulatory focus.
Numerous efforts are underway to implement this model in the United States; NCSBN has an extensive toolkit to assist educators, APNs, consumers, and policymakers implement the new APRN regulatory model (NCSBN, 2012; world wide web.ncsbn.org/2276.htm). The work undertaken to produce the APRN Consensus Model (2008) illustrates the power of interorganizational collaboration and is a promising case of how a model can, equally Fawcett (2005) has suggested, reduce conflicts and facilitate communication inside the profession, beyond professions, and with the public.
American Nurses Association
As the "merely full-service professional organization representing the interests of the nation's three.1 million registered nurses through its constituent and state nurses associations and its organizational affiliates," the American Nurses Clan (ANA) and its constituent organizations accept also been active in developing and promulgating documents that address advanced practice nursing. Two of these are especially of import equally nosotros consider contemporary conceptualizations of advanced practice nursing. Since 1980, ANA has periodically updated its Social Policy Statement (ANA, 2010a). Specialization, expansion, and advancement have consistently been identified as concepts that can differentiate advanced exercise nursing from basic nursing practise. The most recent edition notes that specialization ("focusing on a part of the whole field of professional nursing") can occur at bones or advanced levels and that APNs utilize expanded and specialized cognition and skills in their practices. According to the 2010 statement, expansion, specialization, and avant-garde practice were divers as follows (ANA, 2010a):
ANA'south definitions of specialization and avant-garde do are consistent with the APRN Consensus Model.
ANA likewise establishes and promulgates standards of practice and competencies for RNs and APNs. In the 2d edition of their text, Nursing: Scope and Standards of Practice (ANA, 2010b), 6 standards of practice and sixteen standards of professional functioning are described. Of the 22 standards, one standard outlines additional expectations for APNs compared with RNs; Standard 5, "Implementation," addresses the consultation and prescribing responsibilities of APRNs. Each standard is associated with competencies. Information technology is in the description of the competencies that RN practice is differentiated from APNs and nurses prepared in a specialty at the graduate level. This document is must reading for APN students, practitioners, and others wishing to sympathise how basic, advanced, and specialized practice differ.
In addition to these documents, ANA, together with the American Board of Nursing Specialties (ABNS), convened a job forcefulness on CNS competencies. For many reasons, including the recognition that developing psychometrically sound certifications for numerous specialties, especially for clinical nurse specialists (CNSs), would be difficult as the profession moved toward implementing the APRN Consensus Model, the ANA and ABNS convened a group of stakeholders in 2006 to develop and validate a fix of core competencies that would exist expected of CNSs entering practise (National Clan of Clinical Nurse Specialists [NACNS]/National CNS Cadre Competency Job Strength, 2010). This group was charged with identifying cadre, entry-level competencies that are common in CNS practice, regardless of specialty. This piece of work is discussed afterward in this affiliate in the department on NACNS.
ANA continues to make numerous contributions to promoting clarity about all nursing roles, including advanced practice nursing. Its definitions of expansion, specialization, and avant-garde practice accept remained consistent over time. ANA's Nursing: Scope and Standards of Practice (2010), should inform theoretical and empirical work that aims to differentiate nursing roles.
American Association of Colleges of Nursing
Over the final decade, the AACN has undertaken two nursing didactics initiatives aimed at transforming nursing pedagogy. In 2006, AACN called for all APN training to take place at the doctoral level in practice-based programs (DNP), with master's level education existence refocused on generalist preparation for roles such every bit clinical nurse leaders (CNLs) and staff and clinical educators. CNLs are not APNs (AACN, 2005, 2012a; Spross, Hamric, Hall, et al., 2004) and, therefore, are not included in this word of conceptualizations. Through these initiatives, and to the extent that the AACN and Commission on Collegiate Nursing Education (CCNE) influence accreditation, the DNP may go the preferred degree for most APNs, although this goal is controversial. Since the concluding edition, despite lingering disagreements, DNP educational activity has advanced considerably. In 2006, in that location were xx DNP programs; in 2011, in that location were 182. Similarly, enrollments in and graduation from DNP programs take as well risen substantially (AACN, 2012).
The DNP Essentials (AACN, 2006) are comprised of eight competencies for DNP graduates (Box 2-2). Graduates are expected to demonstrate the eight essentials on graduation. For APNs, "Essential VIII specifies the foundational practice competencies that cut across specialties and are seen as requisite for DNP practice" (AACN, 2006, p. 16; Box 2-three). Recognizing that DNP programs will prepare nurses for roles other than APN roles, the AACN acknowledged that organizations representing APNs are expected to develop Essential VIII as it relates to specific avant-garde practice roles and "to develop competency expectations that build upon and complement DNP Essentials 1 through 8" (AACN, 2006, p. 17). These Essentials affirmed that the advanced practice nursing core includes the three Ps (iii split courses)—avant-garde health and physical assessment, advanced physiology and pathophysiology, and advanced pharmacology—and is specific to APNs. The specialty core must include content and clinical do experiences that help students acquire the knowledge and skills essential to a specific advanced do role. These requirements were reconfirmed in the Consensus Model (2008).
Box ii-3
Essential VIII
Advanced Nursing Practice Competencies
I Conduct a comprehensive and systematic assessment of health and illness parameters in complex situations, incorporating diverse and culturally sensitive approaches.
II Pattern, implement, and evaluate therapeutic interventions based on nursing science and other sciences.
III Develop and sustain therapeutic relationships and partnerships with patients (individual, family, or group) and other professionals to facilitate optimal care and patient outcomes.
Four Demonstrate advanced levels of clinical judgment, systems thinking, and accountability in designing, delivering, and evaluating evidence-based care to better patient outcomes.
V Guide, mentor, and support other nurses to achieve excellence in nursing exercise.
Vi Educate and guide individuals and groups through complex health and situational transitions.
Seven Use conceptual and analytical skills in evaluating the links among practise, organizational, population, fiscal, and policy bug.
From American Association of Colleges of Nursing (AACN). (2006). The essentials of doctoral teaching for advanced nursing practice (www.aacn.nche.edu/publications/position/DNPEssentials.pdf).
The DNP has been described equally a "disruptive innovation" (Hathaway, Jacob, Stegbauer, et al., 2006) and a natural evolution for NP practice. Although the DNP remains controversial (Avery & Howe, 2007; American College of Nurse-Midwives [ACNM], 2012b; Dreher & Smith Glasgow, 2011; Irvin-Lazorko, 2011; NACNS, 2009a), the proposal to brand the DNP required for entry into advanced practice nursing is 1 of several national initiatives that have contributed to a broader discussion and may lead the profession to a clearer definition of advanced practise nursing. One outcome of the national DNP discussion is that APN organizations have promulgated do competencies for doctorally prepared APNs (e.grand., ACNM, 2011c; NACNS, 2009b) or have proposed a practice doctorate, even though it may not exist the DNP (AANA, 2007). The National Organization of Nurse Practitioner Faculties (2012) now has one set of core competencies for NPs. Organizational positions on doctoral education are briefly explored in the word of APN organizations (see later). Readers tin can consult Chapters 14 through xviii and are urged to visit stakeholder organizations' websites for the history and up to date data on organizational responses to AACN's DNP position paper (AACN, 2004) and the DNP Essentials (AACN, 2006).
Although non a conceptual model per se, the AACN'southward publication, DNP Essentials (2006) addresses concepts and content that are now evident in many other documents that address standards of APN practice and educational activity. The fact that Essential VIII affirms a set up of common competencies across APN roles is an important contribution to conceptual clarity about avant-garde exercise in the United States. Because these Essentials, with the exception of Essential VIII, are intended to address DNP preparation for any nursing role, its contribution to conceptual clarity regarding avant-garde exercise nursing specifically is limited. Eventually, the evolution of the DNP may lead to more than conceptual clarity nearly advanced exercise nursing and the office of APNs. However, it is possible that the rapid expansion of this caste may contribute to less clarity in the short term about the nature of advanced nursing practice and the centrality of direct intendance of patients to APN work, particularly because the DNP will prepare people for other, nonclinical nursing roles. In the next department, in addition to discussing the organizations' conceptualizations of APN practise, the extent to which their responses to the DNP proposal might influence conceptual clarity on advanced nursing practice is addressed.
felixhersentooped.blogspot.com
Source: https://nursekey.com/conceptualizations-of-advanced-practice-nursing/
0 Response to "what are the issues related to concepts, models and theories of advanced practice nursing?"
Post a Comment